




profession
Colorectal cancer screening rates rising but still low
■ An NIH panel suggests eliminating financial barriers and implementing interventions to increase screening.
- WITH THIS STORY:
- » Boosting colorectal cancer screening
- » Disparities in screening
- » External links
Colorectal cancer screening rates have been rising nationally over the past decade, but still more needs to be done to reduce prevalence of the disease and related deaths, according to a National Institutes of Health panel.
The 13-member State-of-the-Science Conference panel convened in Bethesda, Md., in early February to analyze national screening rates for colorectal cancer, propose solutions to increase them and identify barriers to screening.
"Randomized trials have shown screening can reduce mortality. But as [the disease] is getting more attention, it's becoming increasingly clear that mortality reductions have fallen short of expectations and what we hoped we'd achieve," said panel member Beth Virnig, PhD, MPH, a professor in the division of health policy and management at the University of Minnesota School of Public Health and co-director of the Cancer Outcomes and Survivorship Research Program at the university's Masonic Cancer Center. "The question is what exactly should be done to increase screening rates."
Among the panel's recommendations: Eliminate financial barriers to screening; implement interventions, such as patient reminder systems; and conduct studies to determine the effectiveness of various screening methods.
Physicians can play an integral role in boosting screening rates.
"Doctors need to recommend screening," Virnig said. "In some cases, they need to push it."
Colorectal cancer deaths
Colorectal cancer is the second leading cause of cancer-related deaths among men and women in the U.S., preceded by lung cancer, according to the American Cancer Society. In 2005, the Centers for Disease Control and Prevention estimated that more than 141,000 people were diagnosed with colorectal cancer, and 53,005 people died from it.
Screening rates for colorectal cancer have been rising among adults age 50 and older for the past decade, growing from approximately 25% of adults in this age group in 1997 to 55% in 2008, according to the NIH. However, the screening rate still falls consistently below those for other types of cancer, particularly breast cancer.
In 2005, 66.5% of women 40 and older received a mammogram within two years, the ACS said. The cancer society recommends women in this age group receive annual mammograms.
Colorectal cancer screening rates also are lower than those for cervical cancer, according to ACS data. A 2005 survey found 79.6% of women 18 and older had received a Pap smear within the previous three years.
One possible reason for the disparity, Virnig said, is the wide variety of colorectal cancer screening methods. There also are varying intervals for screening, ranging from a colonoscopy every 10 years for adults age 50 to 75 to an annual fecal occult blood test, according to recommendations by the U.S. Preventive Services Task Force and the U.S. Multisociety Task Force on Colorectal Cancer. Additionally, the ACS recommends adults 50 and older receive a double-contrast barium enema and computed tomography colonography every five years.
NIH panel members recommend physicians consider a patient's preference when discussing the type of screening method to be used. The panel found the most important factors associated with patients getting screened were insurance coverage and access to a regular health care professional. Removing out-of-pocket costs for tests could increase screening numbers, panel members said.
White adults age 50 and older had the highest screening rate, 62.6%, in 2006, according to the CDC's Behavioral Risk Factor Surveillance System. The lowest rate, 47.2%, was among Hispanic adults. Aiming to close these gaps, panel members recommend doctors target screening strategies for specific populations.
The challenge for physicians is finding the time and resources to educate patients about the multiple screening methods and to issue patient reminders for screening, said Robert Fletcher, MD, professor emeritus of ambulatory care and prevention at Harvard Medical School and former co-chair of the U.S. Multisociety Task Force on Colorectal Cancer.
"There's so much that competes for [primary care physicians'] attention," Dr. Fletcher said. "Sure, they could do screening if that's the only thing they had to do, but they have other things."
ADDITIONAL INFORMATION
Click to see data in PDF.
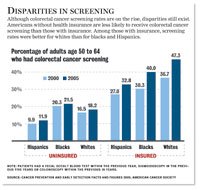
Disparities in screening
Although colorectal cancer screening rates are on the rise, disparities still exist. Americans without health insurance are less likely to receive colorectal cancer screening than those with insurance. Among those with insurance, screening rates were better for whites than for blacks and Hispanics.
Percentage of adults age 50 to 64 who had colorectal cancer screening:
| 2000 | 2005 | |
|---|---|---|
| Uninsured Hispanics | 9.9% | 11.9% |
| Uninsured blacks | 20.3% | 21.5% |
| Uninsured whites | 16.5% | 18.2% |
| Insured Hispanics | 27.0% | 32.8% |
| Insured blacks | 30.3% | 40.0% |
| Insured whites | 36.7% | 47.3% |
Note: Patients had a fecal occult blood test within the previous year, sigmoidoscopy in the previous five years or colonoscopy within the previous 10 years.
Source: Cancer Prevention and Early Detection Facts and Figures 2009, American Cancer Society (link)







