




business

David Blumenthal, MD, the federal government's national coordinator for health information technology, told HIMSS conference attendees that his office will read and listen to all public comments on the interim final rules for EMR certification criteria. Photo courtesy of HIMSS
"Meaningful use" takes time (HIMSS 2010 conference)
■ Guidance on how to earn Medicare EMR pay incentives is available. But experts advise a deliberate approach.
By Pamela Lewis Dolan — Posted April 19, 2010
- WITH THIS STORY:
- » Health IT progress
- » Interest in EMR adoption growing
- » Medicaid incentives available, too
- » Correction
- » Related content
For more than a year, there's been a "hurry up and wait" attitude toward adoption of health information technology, as many doctors delayed buying electronic medical record systems until they got details on how their practices could earn incentive pay for use.
Now that near-final meaningful use criteria have been published, experts and vendors say many doctors are shifting to "hurry up and adopt." But they warn that practices should allow time for the appropriate steps, even as Medicare pay incentives for meaningful use of technology are scheduled to begin in 2011.
Rushing into adoption solely for the sake of earning incentive money is not only a bad business move but also one that could be dangerous to patients, experts warn.
Meaningful use, and physicians' attempts to satisfy the requirements to meet it, was a major topic of discussion at the annual Healthcare Information and Management Systems Society conference, held in March in Atlanta. Physicians, consultants and others described their implementation success stories, most of which involved slow and deliberate processes toward adoption, and warned of failures if that slow and deliberate process is not followed.
The HIMSS conference was held just days before the deadline for organizations to submit comments to the Centers for Medicare & Medicaid Services on the interim final rules that define meaningful use. Several organizations, including HIMSS and the American Medical Association, submitted letters asking CMS to change the rules, claiming that more flexibility and an incremental approach to adoption -- which would help doctors take the baby steps experts recommend -- will help ensure long-term success.
Under the interim final rules, the incentives will be doled out over five years for practices meeting three stages of meaningful use. The first stage includes 25 objectives for physicians and 23 objectives for hospitals to meet to be deemed meaningful EMR users. The objectives include use of computerized physician order entry, e-prescribing and a drug check function for formulary checks, allergies and dangerous drug interactions. Stages 2 and 3 will expand the list of objectives with additions that will be proposed through future rulemaking.
Under the Medicare incentive plan, if physicians meet stage 1 requirements by 2011 or 2012, they can earn a total of $44,000 over five years, starting with $18,000 the first year. But if meeting the requirements takes longer, the totals are lower: $39,000 in 2013 and $24,000 in 2014. The bonuses turn into penalties in 2015 if meaningful use has not been reached.
The release of the interim final rules on EMR system certification was announced at an Office of the National Coordinator town hall meeting at the HIMSS conference. The ONC is accepting comments on those rules.
Not enough time
Experts say there is a long history of practices that deinstalled their systems or didn't get the best use out of them because they weren't careful enough in implementation -- a pattern that could be repeated under the current meaningful use deadlines.
"What we're seeing as we go around the country is a real push to implement. And I have made it my personal mission to say, 'You have to pay attention. This is going to dramatically change the way your organizations do business,' " said Pam Arlotto, CEO and president of Maestro Strategies, a health care consulting firm based in Atlanta.
Arlotto said many medical organizations have concluded that if EMR adoption is done badly, "There will be significant patient safety events." Many experts have said an EMR implementation is a disruptive change in the office. Particularly during the installation period, changes in work flow and tracking of patients can result in unintentional problems. "We can no longer view these as technology implementations alone," she said.
Jeffery Belden, MD, a family physician in a six-doctor practice in Columbia, Mo., and an EMR usability consultant, said many practices have trouble finding EMRs that meet their needs. Finding the right system involves taking each objective and applying usability tests to each one.
"Usability is not just user satisfaction. I think that is the biggest misconception out there," Dr. Belden said. "It has to do with the effectiveness and efficiency of the tool that you are using. Effectiveness means it works consistently, and efficiency means it works, and it doesn't take you a lot longer, and it doesn't give you migraines."
Kathryn Stout, MD, an ob-gyn at the Virginia Women's Center, a physician-owned practice with 38 doctors at five sites in Richmond, said at HIMSS that her practice started looking for an EMR in the mid-1990s but didn't start implementing one until 2004.
After a suitable system was found, implementation took 14 months. Doctors followed a reduced work schedule while the practice redesigned its work flow.
Much discussion centers around doing something voluntarily versus being forced into something, Dr. Stout said. It will be interesting to see "what the results are when we get down to those practices that implement and what kind of functional results they get."
Arguing for more time
CMS is reviewing comments about the new rules. Many organizations said adopting all of the functionalities to qualify a medical practice for stage 1 meaningful use incentives would not be practical or wise in the suggested time frame. Instead of "all-or-nothing" rules, they suggested an incremental approach that would let participants choose which objectives to pursue.
"Successful integration of [electronic medical records] and health IT into patient care takes time and depends on whether or not the methodology employed to achieve integration enhances physician performance and accurately reflects and supports the work of patient care," the American Medical Association wrote in its letter to CMS, which was co-signed by 95 state and specialty medical societies.
In its comment to CMS, the Medical Group Management Assn. went so far as to request a year-long legislative extension of stage 1.
The American Hospital Assn. wants to see a year between finalization of EMR certification criteria and certification of vendor systems. The AHA asked for two more years between the time certified products enter the market and the time health care organizations are expected to meet meaningful use standards for those systems.
Others weighed in, too. The Consumer Partnership for eHealth, a coalition led by the National Partnership for Women & Families, collected perspectives from consumers and employers. Its letter to CMS said the 2011 deadline is too soon and should be scaled back so physicians can focus on simple adoption. "Small primary care practices have fewer resources to implement meaningful use as defined in the proposed rule. Therefore, those intended to benefit the most from these incentives won't," the letter stated. (See correction)
Of significant concern to many of the societies and groups is the required use of computerized physician order entry systems. Stage 1 measures require that 80% of all orders be done through CPOE. Understanding work flow and process changes is an important step of adopting CPOE, the AMA's letter stated.
"We are very concerned that introducing CPOE into the outpatient setting too quickly will create duplicative work for physicians, risk diminished physician-patient communication and may pose patient safety concerns," the AMA wrote.
Maestro Strategies' Arlotto said several health care organizations that are considered technology leaders are not prepared to meet the CPOE objective. "If they don't significantly accelerate their plan ... they probably won't make stage 1 until 2013 or later."
David Blumenthal, MD, national coordinator for health information technology, delivered a keynote address at HIMSS. He gave some organizations hope that their concerns would be heard and acted upon.
"What I'm confident of is that every element in the meaningful use matrix has a direct link to the health of patients, the health of populations or the efficiency of our health care system. If there's any element in that matrix that doesn't have that link, it doesn't belong there," Dr. Blumenthal said. "We are, with all these regulations, going to be hearing your comments. We welcome your comments. We depend on your comments to make these regulations better."
ADDITIONAL INFORMATION
Click to see data in PDF.
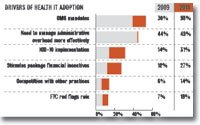
Interest in EMR adoption growing
In 2009, 20% of small practices planned to implement health information technology within 12 months. In 2010, that number is up to 68%, according to a survey by NaviNet, which operates health care communications networks. While the stimulus package and its related incentives play a larger part, it's not the only reason doctors are interested in buying.
Note: Doctors could choose more than one answer.
Source: "Survey: Healthcare Information Technology Adoption Among Small Physician Practices," NaviNet, March (link)







