




profession
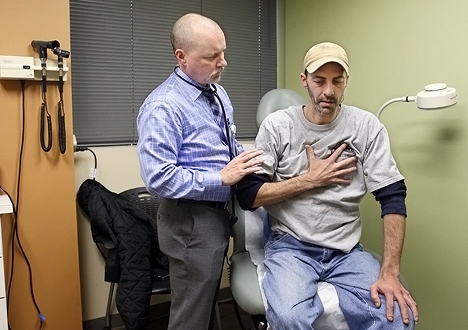
R. Corey Waller, MD, medical director of Spectrum Health System's Center for Integrative Medicine examines Anthony Parish, 39, who had oral surgery in February to alleviate dental pain that had sent him to the emergency department more than 10 times in 2011. When patients call after hours, Dr. Waller will "talk them through the pain" and adjust pain medicines as needed. "A 10-minute conversation saves an ED visit," he says. Photos by Rex Larsen / AP Images for American Medical News
Innovative ways to slash ED overuse
■ Intensive efforts addressing problems that again and again send the same patients to the emergency department are showing promise.
By Kevin B. O’Reilly — Posted April 30, 2012
» View slide show: A new home for frequent ED users
- WITH THIS STORY:
- » Why do patients visit the ED so often?
- » Profile of the frequent ED visitor
- » External links
- » Related content
On a mild, gray day in February, fatigue lined the face of Anthony Parish, a slight, 39-year-old man who has been through a lot. He had a cancerous portion of his lung removed and struggled with postoperative pain. Chemotherapy treatments caused abscesses in his mouth that ruined his teeth and repeatedly sent him to the emergency department for relief, delivered in the form of painkillers and antibiotics.
Despite his health problems, Parish voiced hope on that midwinter morning. His medical team had developed a plan to help alleviate his dental pain. By the end of the month, his infected teeth would be removed and replaced with dentures. He still has intermittent chest pain, but he is learning to cope with it.
Parish is one of about 950 patients identified by Spectrum Health System in Grand Rapids, Mich., as having used their hospital EDs 10 times or more during the previous year. These patients accounted for more than 20,000 total visits and at least $40 million in costs during that period. In November 2011, Spectrum launched the Center for Integrative Medicine, a $1 million multispecialty clinic modeled on a pilot program that slashed ED use by nearly 90%, to help patients like Parish address the source of the problems that keep bringing them back to the ED.
“A lot of doctors, they just say, 'Take this [drug] and see how it goes.' They don't really try to figure out your problems,” Parish says.
That is not the approach he encountered at the center, where Medical Director R. Corey Waller, MD, works with a staff of six to deliver intensive medical and case management interventions to patients over the course of three to six months before transitioning them to primary care physicians in the community or within Spectrum, an integrated health system.
“He solves problems,” Parish says in praise of Dr. Waller.
The Spectrum clinic is part of a fledgling movement to devise new methods to help some of the most challenging patients in medicine — those who visit the ED frequently. The reasons why these patients visit the emergency department vary, and there are no easy fixes. But initiatives that seek to address patients' medical, psychological and social needs are showing promise.
The efforts come as states around the country target emergency department use among Medicaid patients. Democratic Washington Gov. Christine Gregoire suspended a plan that was set to take effect April 1 and would have restricted Medicaid pay to EDs for more than 400 conditions. The American Medical Association was among the physician organizations that objected to the policy.

Spectrum social worker Dennis Potter helps patients form a long-term plan to address problems and keep them out of the ED.
Meanwhile, starting in October, hospitals face up to 1% in Medicare pay cuts for high readmission rates. That penalty threat is giving hospitals another incentive to do what they can to help patients avoid the ED.
Understanding repeat ED users
There is no standard definition for what constitutes frequent emergency department use, but researchers set four or more annual visits as a cutoff. The 8% of patients who use the emergency department four-plus times a year account for 28% of adult ED visits, according to a July 2006 Annals of Emergency Medicine study.
Compared with patients who use the ED less often, frequent users are much likelier to have poor physical health and live below the poverty threshold, said the study, based on a nationally representative household survey. Frequent ED users are more likely to be uninsured or publicly insured and 70% likelier to have poor mental health. And these patients do not rely solely on the emergency department; they are three times more likely to have made five or more outpatient visits in the last year.
“These are patients with needs,” says Ellen J. Weber, MD, co-author of the Annals study. “They're chronically ill. They have mental illnesses that may make it harder for them to manage their physical illnesses. They also are frequent users of other aspects of the health system. These are not patients who are using the ED instead of the outpatient care system. These are patients who are using it along with everything else the health care system has to offer.”
The notion that most frequent ED users are abusing the system is not backed by evidence, says Dr. Weber, professor of clinical emergency medicine at the University of California, San Francisco School of Medicine.
“They're not necessarily coming to the ED because it's easier or convenient, or for minor reasons,” she says.
Maria C. Raven, MD, MPH, agrees.
“People aren't coming to just hang out,” says Dr. Raven, assistant professor of clinical emergency medicine at UCSF. “They've got some real issue that's bringing them in. They're scared.”
Coordinating care is critical
Before coming to UCSF, Dr. Raven helped start a pilot program at New York City's Bellevue Hospital Center that enrolled 19 patients who had a total of 106 ED visits and 64 hospital admissions in the previous year. Of the 19 patients, all men, 18 had substance-abuse problems and 17 were homeless. The hospital hired a care manager to coordinate care inside and outside the hospital.
In-depth interviews at the bedside identify the patients' housing, transportation and medical needs such as substance-abuse rehabilitation. Instead of discharging patients to the streets, staffers work to find permanent housing and put them up at the YMCA while housing applications get processed. Often, patients are given prepaid cellphones to facilitate planning.
Weekly conference calls with primary care doctors, visiting nurse services, methadone programs, substance abuse programs and others are conducted to make sure everyone is “on the same page,” Dr. Raven says. Overall, ED visits were cut by 10%, and hospitalizations were slashed by nearly 40%, according to results published Oct. 13, 2011, in BMC Health Services Research.
“One of the most problematic things is that the medical side of things is not well-aligned with the mental and behavioral-health services, and things are often very fragmented,” Dr. Raven says. “There's not really the ability for the medical system to communicate with the welfare system.”
Without help, it is difficult for physicians in the hospital to address the root cause of what is bringing patients back to the ED so often, she adds.
“Often where things break down during the hospital or ED visit is that the medical team working with these patients may not know them or what's going on with them outside of the hospital,” Dr. Raven says. “There's pressure to get them out of the hospital, depending on the payment structure. They sort of do what they can to wrap up the individual episode of care neatly and discharge the patient. There's not someone doing the simple things like postdischarge follow-up with a phone call.”
The program has been expanded to a total of three hospitals that are part of the New York City Health and Hospitals Corp. and is being funded by the state's Medicaid plan to prevent costly ED and hospital use.
In neighboring New Jersey, a nonprofit effort chronicled in The New Yorker and on TV's “Frontline” is targeting frequent emergency department users in the city of Camden. In 2007, the physician-led Camden Coalition of Healthcare Providers organized a collaborative of primary care, behavioral health and social service professionals to help these patients avoid the ED. Among the first 36 patients identified for extra help, the total average monthly number of hospital and ED visits dropped from 62 to 37, a 40% cut. Meanwhile, hospital bills were slashed by 56%.
Rerouting frequent ED users
These fledgling quality initiatives are not only critical to improving patients' lives and controlling health care costs, but to sustaining the morale of emergency physicians. A survey of more than 400 emergency physicians presented at the Society for Academic Emergency Medicine's June 2011 annual meeting found that about 60% reported having less empathy for patients who use the ED more than 10 times a year, sometimes derisively dubbed “frequent fliers.” Experts fear that hardening of the heart could translate into worse patient care.
And while nearly all the emergency doctors reported experience with frequent ED users, only 30% said they work in a hospital that has a program dedicated to helping these patients avoid the hospital through programs involving case managers and social workers.
Dr. Waller, of the Spectrum Center for Integrative Medicine in Grand Rapids, said he grew so frustrated during his time working in the emergency department that he considered quitting medicine. He never had the time to delve deeply into the complex conditions that were bringing patients back to the ED so often. And most frequent ED users have a constellation of physical and mental illnesses that go beyond the scope of emergency medicine, he says.
“If you've been smashed by a truck, or you have a laceration from the top of the chest to the bottom of the toe, that's perfect for the ER,” says Dr. Waller, who also specializes in addiction and pain medicine. “What it's not perfect for is someone with a chronic, debilitating mental-health disorder who shows up and is seen by a physician who's had one lecture on that in their entire training.”
So far, the center has seen about 100 high-volume ED patients, and about a third have been completely stabilized and transferred to a primary care physician. Other patients randomly wait-listed for the clinic's services act as a control to determine the effectiveness in reducing ED visits. The first visit to the clinic can last as long as four or five hours, with patients seeing a case manager and then a medical social worker before visiting Dr. Waller for a complete work-up.
The vast majority of the center's patients have chronic pain and mental health problems, and the goal is to find the medical source of the pain and address it directly. Patients sometimes have major undiagnosed conditions such as Crohn's disease or spinal pathology, or simply have poorly managed chronic conditions. For patients with no discernible source of pain, Dr. Waller works to wean them off opiates by using buprenorphine and similar medications. Meanwhile, patients receive counseling on how to use cognitive-behavioral and other techniques to cope with the aches, pains and stressors of daily life.
“We have no official appointments,” says Dennis Potter, one of the center's social workers. “We just want to give patients a chance to hang out and talk through what's going on in their lives. It's designed to relieve the anxiety or the issues they're bringing in, and hopefully assist them in learning that every time you're in distress, it doesn't mean you have to go to the ED. Every time you have a pain, it doesn't mean you have to have a pill.”
Patients who use the ED frequently deserve better care than what they typically get, Dr. Waller says.
“These are patients who have been marginalized, verbally beaten in the hospital and called drug addict, dirt bag, drug seeker. Those are terms I've heard from my colleagues about these patients, and it made me angry and it's not right,” he says.
“It's really fulfilling to do the right thing for a patient, where the last time you saw that patient in the ER they hated you and the next time they hug you and say, 'Thank you for helping me.' Doing the right thing is the right thing to do. It's not just a theory.”







